Prostate Cancer
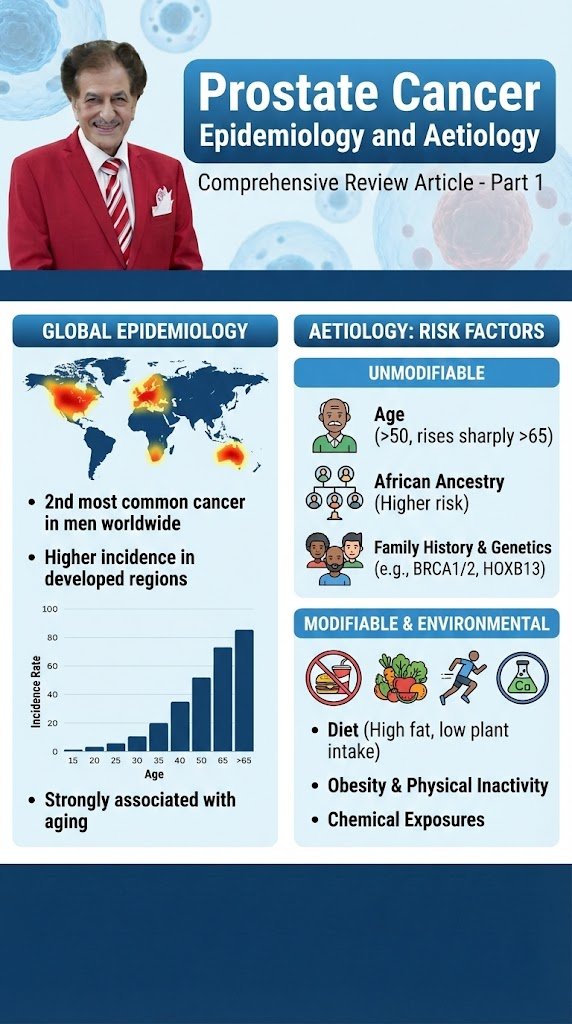
Prostate Cancer Epidemiology and Aetiology Comprehensive Review Article Part 1 Prof. Dr. Semir. A. Salim. Al Samarrai Prostate cancer is the second most commonly diagnosed cancer in men, with an estimated 1.4 million diagnoses worldwide in 2020 [1,2]. The frequency of autopsy-detected PCa is roughly the same worldwide [3]. A systematic review of autopsy studies reported a prevalence of PCa at age < 30 years of 5% (95% confidence interval [CI]: 3–8%), increasing by an odds ratio (OR) of 1.7 (1.6–1.8) per decade, to a prevalence of 59% (48–71%) by age > 79 years [4]. The incidence of PCa diagnosis varies widely between different geographical areas, being highest in Australia/New Zealand and Northern America (age-standardised rates [ASR] per 100,000 of 111.6 and 97.2, respectively), and in Western and Northern Europe (ASRs of 94.9 and 85, respectively), largely due to the use of prostate-specific antigen (PSA) testing and the aging population. The incidence is low in Eastern and South-Central Asia (ASRs of 10.5 and 4.5, respectively), but rising [5]. Rates in Eastern and Southern Europe were low but have also shown a steady increase [2,3]. Incidence and disease stage distribution patterns follow biological-, genetic-, and/or lifestyle factors [6]. There is relatively less variation in mortality rates worldwide, although rates are generally high in populations of African descent (Caribbean: ASR of 29 and Sub-Saharan Africa: ASRs ranging between 19 and 14), intermediate in the USA and very low in Asia (South-Central Asia: ASR of 2.9) [2]. Family history and ethnic background are associated with an increased PCa incidence suggesting a genetic predisposition [7,8]. Only a small subpopulation of men with PCa have true hereditary disease. Hereditary PCa (HPCa) is associated with a six to seven year earlier disease onset but the disease aggressiveness and clinical course does not seem to differ in other ways [7,9]. In a large USA population database, HPCa (in 2.18% of participants) showed a relative risk (RR) of 2.30 for diagnosis of any PCa, 3.93 for early-onset PCa, 2.21 for lethal PCa, and 2.32 for clinically significant PCa (csPCa) [10]. These increased risks of HPCa were higher than for familial PCa (> 2 first- or second-degree relatives with PCa on the same side of the pedigree), or familial syndromes such as hereditary breast and ovarian cancer and Lynch syndrome. The probability of high-risk PCa at age 65 was 11.4% (vs. a population risk of 1.4%) in a Swedish population-based study [11]. The Identification of Men with a Genetic Predisposition to Prostate Cancer (IMPACT) study, which evaluated targeted PCa screening (annually, biopsy recommended if PSA > 3.0 ng/mL) using PSA in men aged 40–69 years with germline BRCA1/2 mutations found that after 3 years of screening, BRCA2 mutation carriers were associated with a higher incidence of PCa, a younger age of diagnosis, and more clinically significant tumours compared with non-carriers [12]. The influence of BRCA1 mutations on PCa remained unclear. No differences in age or tumour characteristics were detected between BRCA1 carriers and BRCA1 non-carriers. Limitations of the IMPACT study include the lack of magnetic resonance imaging (MRI) data and targeted biopsies as it was initiated before that era. A wide variety of exogenous/environmental factors have been discussed as being associated with the risk of developing PCa or as being aetiologically important for the progression from latent to clinical PCa [13]. Japanese men have a lower PCa risk compared to men from the Western world. However, as Japanese men move from Japan to California, their risk of PCa increases, approaching that of American men, implying a role of environmental or dietary factors [14]. However, currently there are no known effective preventative dietary or pharmacological interventions. The single components of metabolic syndrome (MetS), hypertension (p = 0.035) and waist circumference > 102 cm (p = 0.007), have been associated with a significantly greater risk of PCa. The association between metformin use and PCa is controversial. At population level, metformin users (but not other oral hypoglycaemic agents) were found to be at a decreased risk of PCa diagnosis compared with neverusers (adjusted OR: 0.84, 95% CI: 0.74–0.96) [15]. In 540 diabetic participants of the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) study, metformin use was not significantly associated with PCa and therefore not advised as a preventive measure (OR: 1.19, p = 0.50) [16]. The ongoing Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy (STAMPEDE) trial assesses metformin use in advanced PCa (Arm K) [17]. Figure 1. Risk Factors of Prostatic Cancer. A meta-analysis of 14 large prospective studies did not show any association between blood total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol levels and the risk of either overall PCa or high-grade PCa [18]. Results from the REDUCE study also did not show a preventive effect of statins on PCa risk [19]. Within the REDUCE study, obesity was associated with lower risk of low-grade PCa in multivariable analyses (OR: 0.79, p = 0.01), but increased risk of high-grade PCa (OR: 1.28, p = 0.042) [20]. This effect seems mainly explained by environmental determinants of height/body mass index (BMI) rather than genetically elevated height or BMI [21]. The association between a wide variety of dietary factors and PCa have been studied, but there is paucity of quality of evidence (table 1). Table 1. Main dietary factors that Have been associated with PCa Although it seems that 5-ARIs have the potential of preventing or delaying the development of PCa (~25%, for ISUP grade 1 cancer only), this must be weighed against treatment-related side effects as well as the potential small increased risk of high-grade PCas, although these do not seem to impact PCa mortality [39–42]. None of the available 5-ARIs have been approved by the European Medicines Agency (EMA) for chemoprevention. Hypogonadal men receiving testosterone supplements do not have an increased risk of PCa [43]. A pooled analysis showed that men with very low concentrations of free testosterone (lowest 10%) have a belowaverage risk (OR: 0.77) of PCa [44]. A significantly higher rate of ISUP
Prostate Cancer قراءة المزيد »