Non-muscle-invasive Bladder Cancer
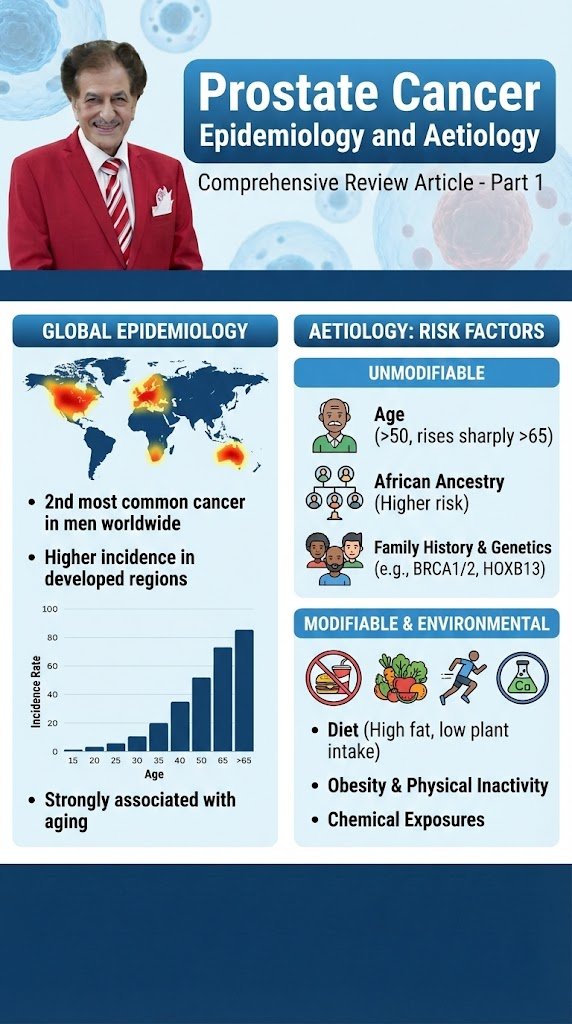
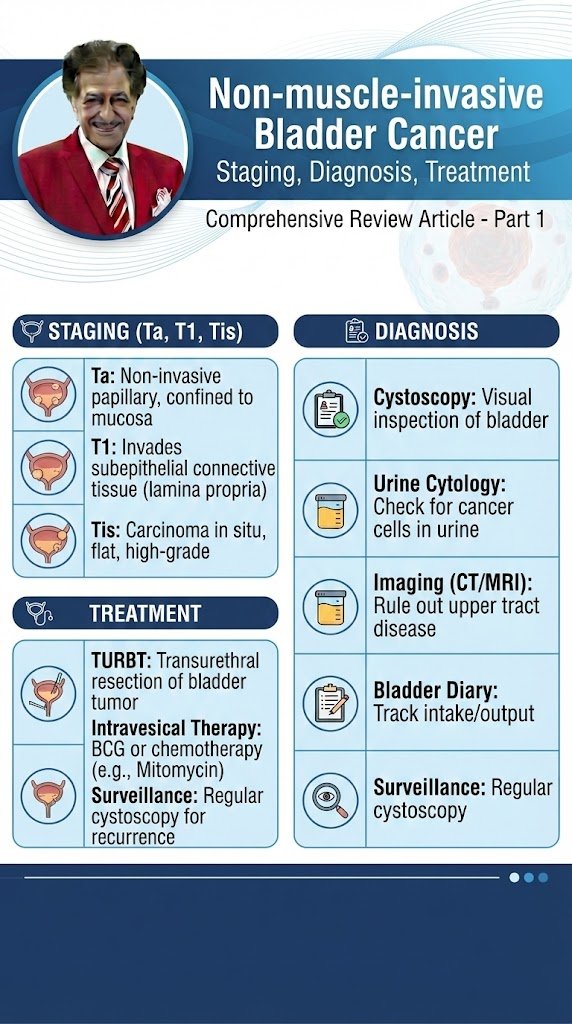
Non-muscle-invasive Bladder Cancer Part 1 Comprehensive Review Article Prof. Dr. Semir. A. Salim. Al Samarrai EPIDEMIOLOGY, AETIOLOGY AND PATHOLOGY: Epidemiology Bladder cancer (BC) is the seventh most commonly diagnosed cancer in the male population worldwide, while it drops to tenth when both genders are considered [1]. The worldwide age-standardised incidence rate (per 100,000 person/years) is 9.5 in men and 2.4 in women [1]. In the European Union the age-standardised incidence rate is 20 for men and 4.6 for women [1]. Worldwide, the BC age-standardised mortality rate (per 100,000 person/years) was 3.3 for men vs. 0.86 for women [1]. Bladder cancer incidence and mortality rates vary across countries due to differences in risk factors, detection and diagnostic practices, and availability of treatments. The variations are, however, partly caused by the different methodologies used and the quality of data collection [2]. The incidence and mortality of BC has decreased in some registries, possibly reflecting the decreased impact of causative agents [3]. Approximately 75% of patients with BC present with a disease confined to the mucosa (stage Ta, CIS) or submucosa (stage T1); in younger patients (< 40 years of age) this percentage is even higher [4]. Patients with TaT1 and CIS have a high prevalence due to long-term survival in many cases and lower risk of cancer-specific mortality compared to T2-4 tumours [1,2]. Aetiology Tobacco smoking is the most important risk factor for BC, accounting for approximately 50% of cases [2,3, 5–7]. The risk of BC increases with smoking duration and smoking intensity [6]. Low-tar cigarettes are not associated with a lower risk of developing BC [6]. The risk associated with electronic cigarettes is not adequately assessed; however, carcinogens have been identified in urine [8]. Environmental exposure to tobacco smoke is also associated with an increased risk of BC [2]. Tobacco smoke contains aromatic amines and polycyclic aromatic hydrocarbons, which are renally excreted. Occupational exposure to aromatic amines, polycyclic aromatic hydrocarbons and chlorinated hydrocarbons is the second most important risk factor for BC, accounting for about 10% of all cases. This type of occupational exposure occurs mainly in industrial plants which process paint, dye, metal, and petroleum products [2, 3, 9, 10]. In developed industrial settings these risks have been reduced by work-safety guidelines; therefore, chemical workers no longer have a higher incidence of BC compared to the general population [2, 9, 10]. Recently, greater occupational exposure to diesel exhaust has been suggested as a significant risk factor (odds ratio [OR]: 1.61; 95% confidence interval [CI]: 1.08–2.40) [11]. While family history seems to have little impact [12] and, to date, no overt significance of any genetic variation for BC has been shown; genetic predisposition has an influence on the incidence of BC via its impact on susceptibility to other risk factors [2, 13–17]. This has been suggested to lead to familial clustering of BC with an increased risk for first- and second-degree relatives (hazard ratio [HR]: 1.69; 95% CI: 1.47−1.95) [18]. Although the impact of drinking habits is uncertain, the chlorination of drinking water and subsequent levels of trihalomethanes are potentially carcinogenic, also exposure to arsenic in drinking water increases risk [2, 19]. Arsenic intake and smoking have a combined effect [20]. The association between personal hair dye use and risk remains uncertain; an increased risk has been suggested in users of permanent hair dyes with a slow NAT2 acetylation phenotype [2] but a large prospective cohort study could not identify an association between hair dye and risk of most cancer and cancer-related mortality [21]. Dietary habits seem to have limited impact, recently protective impact of flavonoids has been suggested and a Mediterranean diet, characterised by a high consumption of vegetables and non-saturated fat (olive oil) and moderate consumption of protein, was linked to some reduction of BC risk (HR: 0.85, 95% CI: 0.77−0.93) [22–27]. The impact of an increased consumption of fruits has been suggested to reduce the risk of BC; to date, this effect has been demonstrated to be significant in women only (HR: 0.92; 95% CI: 0.85–0.99) [28]. Exposure to ionizing radiation is connected with increased risk; a weak association was also suggested for cyclophosphamide and pioglitazone [2, 19, 29]. The impact of metabolic factors (body mass index, blood pressure, plasma glucose, cholesterol, and triglycerides) is uncertain [30]. Schistosomiasis, a chronic endemic cystitis based on recurrent infection with a parasitic trematode, is also a cause of BC [2]. PATHOLOGICAL STAGING AND CLASSIFICATION SYSTEMS: Definition of non-muscle-invasive bladder cancer LE 2a 3 3 Tumours confined to the mucosa and invading the lamina propria are classified as stage Ta and T1, respectively, according to the Tumour, Node, Metastasis (TNM) classification system [31]. Intra-epithelial, highgrade (HG) tumours confined to the mucosa are classified as CIS (Tis). All of these tumours can be treated by transurethral resection of the bladder (TURB), eventually in combination with intravesical instillations and are therefore grouped under the heading of NMIBC for therapeutic purposes. The term ‘non-muscle-invasive BC’ represents a group definition and all tumours should be characterised according to their stage, grade, and further pathological characteristics. Tumour, Node, Metastasis Classification (TNM) The latest TNM classification approved by the Union International Contre le Cancer (UICC) (8th Edn.) is referred to (Table 1) [31]. Table 1: 2017 TNM classification of urinary bladder cancer T1 subclassification The depth and extent of invasion into the lamina propria (T1 sub-staging) has been demonstrated to be of prognostic value in retrospective cohort studies [32, 33]. Its use is recommended by the most recent 2016 World Health Organization (WHO) classification [34]. T1 sub-staging methods are based either on micrometric (T1e and T1m) or histo-anatomic (T1a and T1b) principles; the optimal classification system, however, remains to be defined [34, 35]. Carcinoma in situ and its classification Carcinoma in situ is a flat, HG, non-invasive urothelial carcinoma. It can be missed or misinterpreted as an inflammatory lesion during cystoscopy if not biopsied. Carcinoma in situ is often multifocal and can occur in the bladder, but also in the upper urinary tract (UUT), prostatic ducts, and
Non-muscle-invasive Bladder Cancer قراءة المزيد »