Prostate Cancer
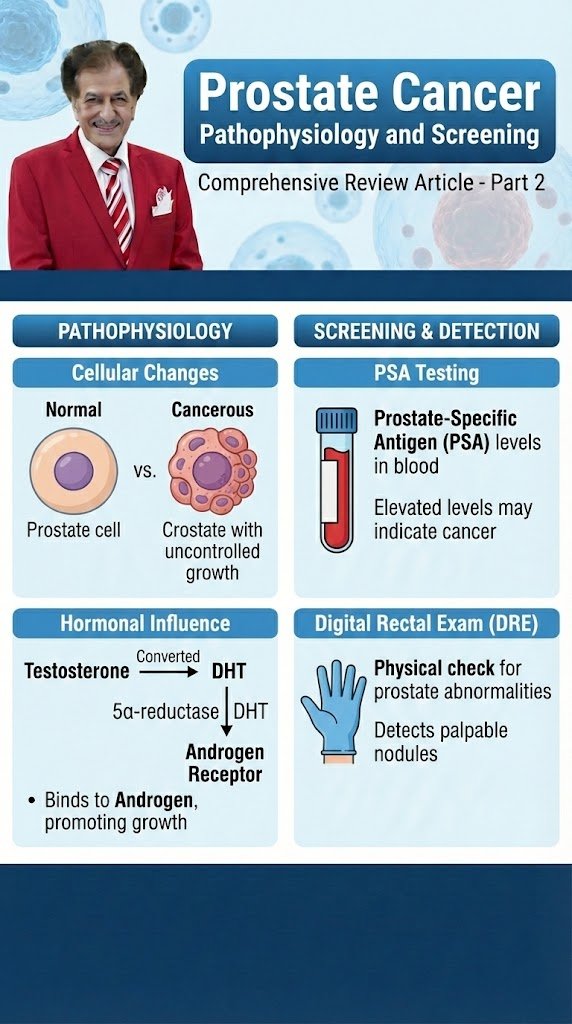
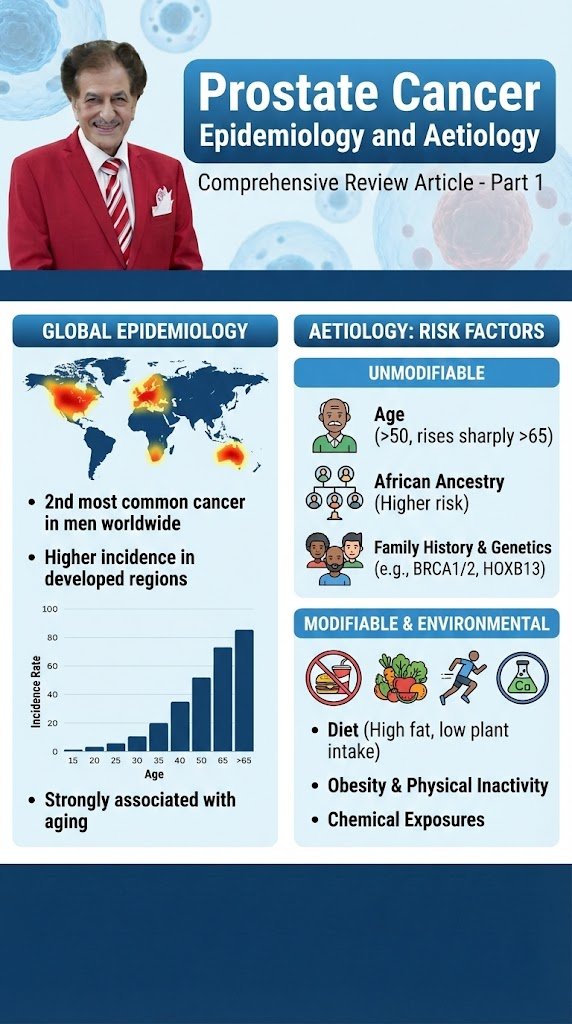
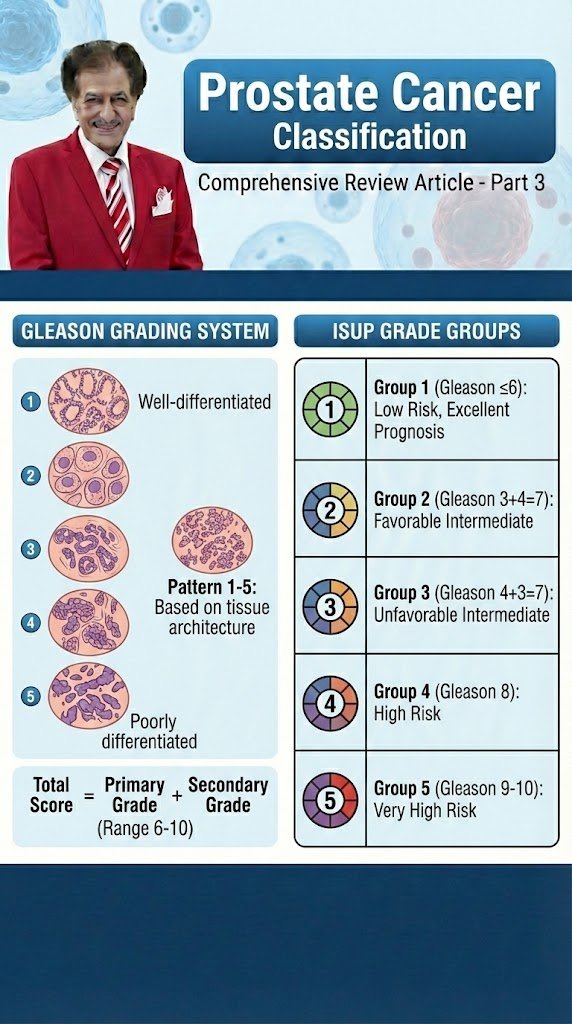
Prostate Cancer Diagnostic Evaluation Comprehensive Review Article Part 3 Prof. Dr. Semir. A. Salim. Al Samarrai Figure 1. Schematic representation of traditional and proposed mpMRI-molecular-biomarker-directed prostate cancer diagnostic pathway. CaP, prostate cancer; PSA, prostate serum antigen; DRE, digital rectal examination; mpMRI, multiparametric magnetic resonance imaging. Text color of FDA/CLIA-approved molecular markers represents tissue of origin: yellow—urine derived; red—blood derived; brown—tissue derived. The diagnostic evaluations are a very important measures in the screening and early detection of prostate cancer in decreasing of cancer-specific mortality by developing early and precise treatment and strategy. Prostate cancer mortality trends range widely from country to country in the industrialised world [1]. Mortality due to PCa has decreased in most Western nations but the magnitude of the reduction varies between countries. The integration of MRI in the biopsy protocol may reduce the number of men that undergo biopsies while detecting more clinically significant and less clinically insignificant PCa [2,3]. Men at elevated risk of having PCa are those > 50 years [4] or at age > 45 years with a family history of PCa (either paternal or maternal) [5] or of African descent [6,7]. Men of African descent are more likely to be diagnosed with more advanced disease [8] and upgrade was more frequent after prostatectomy as compared to Caucasian men (49% vs. 26%) [9]. Germline mutations are associated with an increased risk of the development of aggressive PCa, i.e. BRCA2 [10,11]. Prostate-specific antigen screening in male BRCA1 and 2 carriers detected more significant cancers at a younger age compared to non-mutation carriers [12,13]. Men with a baseline PSA < 1 ng/mL at 40 years and < 2 ng/mL at 60 years are at decreased risk of PCa metastasis or death from PCa several decades later [14,15]. Informed men requesting an early diagnosis should be given a PSA test and undergo a DRE [16]. The use of DRE alone in the primary care setting had a sensitivity and specificity below 60%, possibly due to in experience, and can therefore not be recommended to exclude PCa [17]. Prostate-specific antigen measurement and DRE need to be repeated [18]. This could be every 2 years for those initially at risk, or postponed up to 8 years in those not at risk with an initial PSA < 1 ng/mL at 40 years and a PSA < 2 ng/mL at 60 years of age and a negative family history [19]. Risk calculators, combining clinical data (age, DRE findings, PSA level, etc.) may be useful in helping to determine (on an individual basis) what the potential risk of cancer may be, thereby reducing the number of unnecessary biopsies. Prostate MRI stratifies suspected PCa in lower- and higher risk, based on a 1- to 5- risk scale of having csPCa [PI-RADS v2.1 guidelines 2019]. A recent meta-analysis of this risk assessment tool showed (on a patient level) a significant cancer detection rate of 9% (5–13%) for PI-RADS 2 scores, 16% (7–27%) for PI-RADS 3 scores, 59% (39–78%) for PI-RADS 4 scores, and 85% (73–94%) for PI-RADS 5 scores [20]. Men with PI-RADS assessment scores of 3 to 5 are recommended to undergo biopsy [21]. Prostate MRI and related MRI-directed biopsies have shown to be at least as diagnostically effective as systematic biopsies alone in diagnosing significant cancers [22]. However, if the MRI-directed biopsy decision strategy (without performing systematic biopsies) can reduce the number of unnecessary biopsy procedures, this will be at the expense of missing a small percentage of csPCas [23]. PSA-density (PSA-D) is the strongest predictor in risk calculators. Combinations of PSA-D and MRI have been explored [24-29], showing guidance in biopsy-decisions whilst safely avoiding redundant biopsy testing. Increasing evidence supports the implementation of genetic counselling and germline testing in early detection and PCa management [30]. Several commercial screening panels are now available to assess main PCa risk genes [31]. However, it remains unclear when germline testing should be considered and how this may impact localised and metastatic disease management. Germline BRCA1 and BRCA2 mutations occur in approximately 0.2% to 0.3% of the general population [32]. It is important to understand the difference between somatic testing, which is performed on the tumour, and germline testing, which is performed on blood or saliva and identifies inherited mutations. Genetic counselling is required prior to and after undergoing germline testing. Germline mutations can drive the development of aggressive PCa. Therefore, the following men with a personal or family history of PCa or other cancer types arising from DNA repair gene mutations should be considered for germline testing: • Men with metastatic PCa; • Men with high-risk PCa and a family member diagnosed with PCa at age < 60 years; • Men with multiple family members diagnosed with csPCa at age < 60 years or a family member who died from PCa cancer; • Men with a family history of high-risk germline mutations or a family history of multiple cancers on the same side of the family. Further research in this field (including not so well-known germline mutations) is needed to develop screening, early detection and treatment paradigms for mutation carriers and family members (table 1). Table 1. Germline mutations in DNA repair genes associated with increased risk of prostate cancer By the clinical diagnosis evaluation, prostate cancer is usually suspected on the basis of DRE and/or PSA levels. Definitive diagnosis depends on histopathological verification of adenocarcinoma in prostate biopsy cores. In ~18% of cases, PCa is detected by suspect DRE alone, irrespective of PSA level [50]. A suspect DRE in patients with a PSA level < 2 ng/mL has a positive predictive value (PPV) of 5–30% [51]. The use of PSA as a serum marker has revolutionised PCa diagnosis [52]. Prostate-specific antigen is organ but not cancer specific; therefore, it may be elevated in benign prostatic hypertrophy (BPH), prostatitis and other non-malignant conditions. As an independent variable, PSA is a better predictor of cancer than either DRE or TRUS [53]. There are no agreed standards defined for measuring PSA [54]. It is a continuous parameter,
Prostate Cancer قراءة المزيد »