Overactive Urinary Bladder
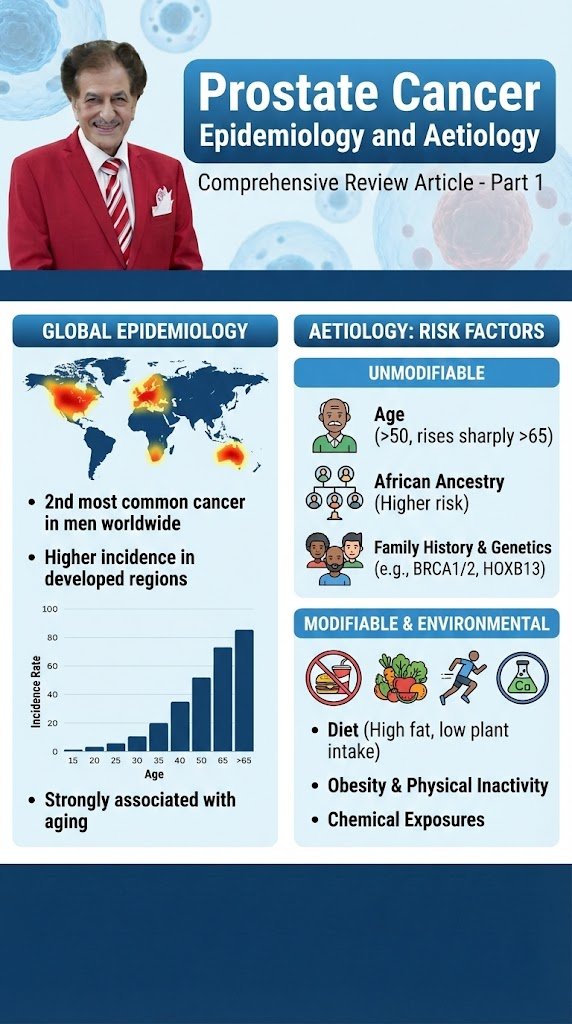
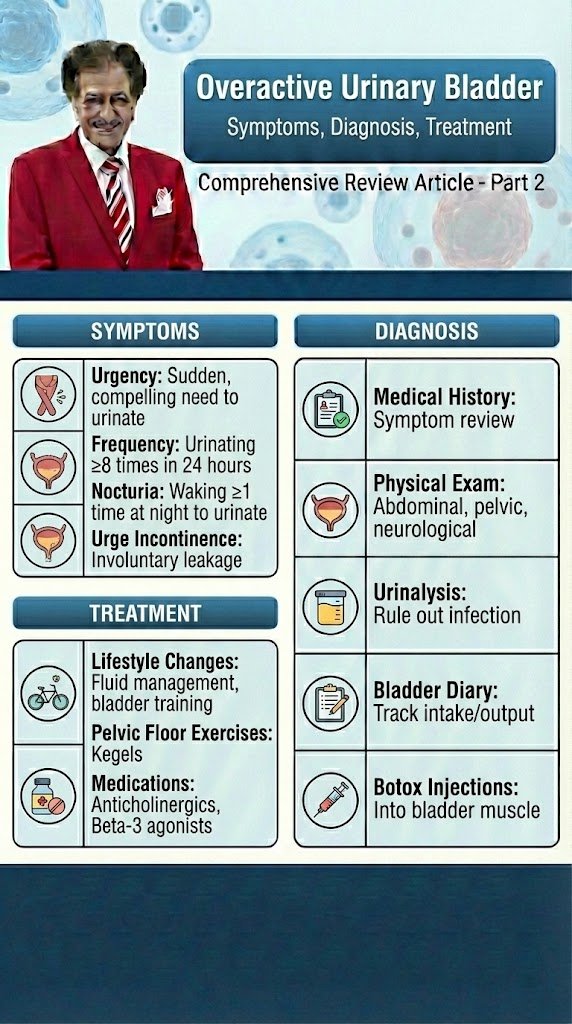
Overactive Urinary Bladder Diagnostic and Evaluation Comprehensive Review Article Part 2 Prof. Dr. Semir. A. Salim. Al Samarrai Taking a thorough clinical history is fundamental to the process of clinical evaluation. Despite the lack of high-level evidence to support taking a history, there is universal agreement that it should be the first step in the assessment of anyone with lower urinary tract symptoms (LUTS). The history should include a full evaluation of LUTS, as well as sexual, gastrointestinal and neurological symptoms. Details of urgency episodes, the type, timing and severity of urinary incontinence (UI), and some attempt to quantify symptoms should also be made. The history should help to categorise LUTS as storage, voiding and post-micturition symptoms, and classify UI as stress urinary incontinence (SUI), urge urinary incontinence (UUI), mixed urinary incontinence (MUI) or overflow incontinence; the latter being defined as “the complaint of UI in the symptomatic presence of an excessively (over-) full bladder (no cause identified)” [1]. The history should also identify patients who need referral to an appropriate clinic/specialist. These may include patients with associated pain, haematuria, history of recurrent urinary tract infection (UTI), pelvic surgery or radiotherapy, constant leakage suggesting a fistula, new-onset enuresis or suspected neurological disease. A neurological, obstetric and gynaecological history may help to understand the underlying cause and identify factors that may affect treatment decisions. Guidance on history-taking and diagnosis in relation to UTIs, neuro-urological conditions and chronic pelvic pain (CPP) can be found in the relevant EAU Guidelines [2,3,4]. Patients should also be asked about other comorbidity as well as smoking status, previous surgical procedures and current medications, as these may affect LUTS. There is little evidence from clinical trials that carrying out a clinical examination improves outcomes, but widespread consensus suggests that clinical examination remains an essential part of assessment of patients with LUTS. Examination should include abdominal examination, to detect an enlarged urinary bladder or other abdominal mass, and digital examination of the vagina and/or rectum. Pelvic examination in women includes assessment of oestrogen status, pelvic floor muscle (PFM) function and careful assessment of any associated pelvic organ prolapse (POP). A cough stress test is necessary to look for stress urinary incontinence (SUI). Among women with genital prolapse, the cough test was found to show good agreement with urodynamic studies (UDS) in the detection of SUI. Urethral mobility can be assessed. Pelvic floor muscle contraction strength can also be assessed digitally. A focused neuro-urological examination should also be routinely undertaken. Patient questionnaires include symptom scores, symptom questionnaires/scales/indices, patient-reported outcome measures (PROMs) and health-related quality of life (QoL) measures. Questionnaires should have been validated for the language in which they are being used, and, if used for outcome evaluation, should have been shown to be sensitive to change. The US Food and Drug Administration (FDA) published guidance for industry on PROM instruments (questionnaires) in 2009 [5]. Patient bladder diaries include measurement of the frequency and severity of LUTS and is an important step in the evaluation and management of LUT dysfunction. Bladder diaries are a semi-objective method of quantifying symptoms, such as frequency of urinary incontinence (UI) events, number of nocturia episodes, etc. Fluid intake and voided volume measurement can be used to support diagnoses and management planning, for example in overactive bladder (OAB), and for identifying 24-hour or nocturnal polyuria. The optimum number of days required for bladder diaries appears to be based on a balance between accuracy and compliance [6,7]. Diary durations between three and seven days are routinely reported in the literature. The urinalysis and urinary tract infection investigations are a very important steps in the evaluation and therapy of UTI. Reagent strip (dipstick) urinalysis may indicate proteinuria, haematuria or glycosuria, or suggest UTI requiring further assessment. Urine dipstick testing is a useful adjunct to clinical evaluation in patients in whom urinary symptoms are suspected to be due to UTI. Urinalysis negative for nitrite and leukocyte esterase may exclude bacteriuria in women with LUTS [8], and should be included, with urine culture when necessary, in the evaluation of all patients with LUTS. Urinary incontinence or worsening of LUTS may occur during UTI [9] and existing UI may worsen [10]. The rate and severity of UI were unchanged after eradication of asymptomatic bacteriuria in nursing home residents [11]. The post-void residual volume measurement is also important step in the evaluation and management of OAB and obstruction LUT-Disorders. Post-void residual (PVR) volume is the amount of urine that remains in the bladder after voiding. It is a measure of voiding efficiency, and results from a number of contributing factors. The detection of significant PVR volume is important because it may worsen symptoms and, more rarely, may be associated with UTI, upper urinary tract (UUT) dilatation and renal insufficiency. Both BOO and/or detrusor underactivity (DU) can potentially contribute to the development of significant PVR volume. Post-void residual volume can be measured by catheterisation or ultrasound (US). Most studies investigating PVR volume have assessed mixed populations including those with neurogenic UI. In general, the data on PVR volume can be applied with caution to women with non-neurogenic LUTS. The results of studies investigating the best method of measuring PVR volume [11-16] have led to the consensus that US measurement of PVR volume is preferable to catheterisation due to its favourable risk–benefit profile. In peri- and postmenopausal women without significant LUTS or pelvic organ symptoms, 95% had a PVR volume < 100 mL [17]. In women with UUI, PVR volume > 100 mL was found in only 10% of cases [18]. Other research has found that a high PVR volume is associated with pelvic organ prolapse (POP), voiding symptoms and an absence of SUI [17, 19–21]. In women with SUI, the mean PVR volume was 39 mL measured by catheterisation and 63 mL measured by US, with 16% of women having PVR volume > 100 mL [22]. Some authors have suggested that it is reasonable to consider a PVR volume > 100 mL to be significant, although many women may remain
Overactive Urinary Bladder قراءة المزيد »