Benign Prostatic Enlargement
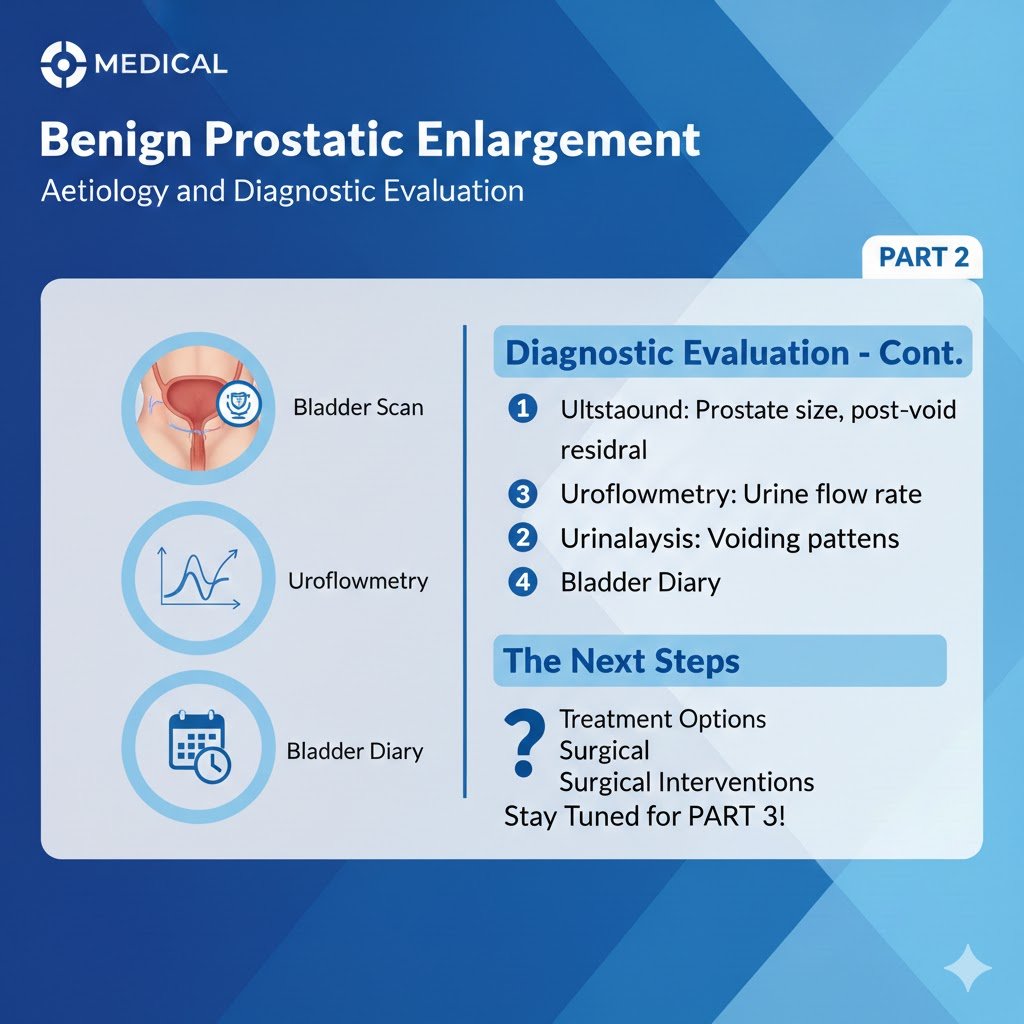
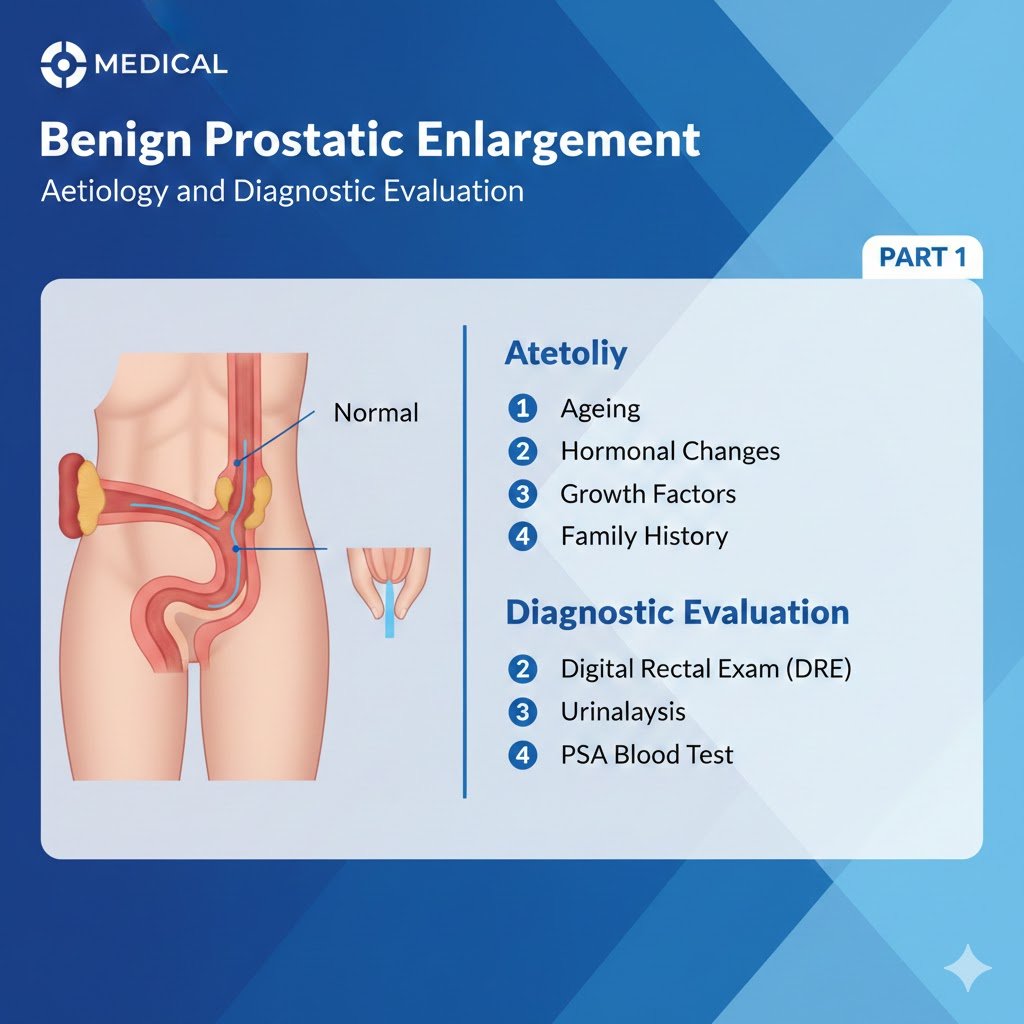
Benign Prostatic Enlargement Surgical Therapy PART 3 Comprehensive Review Article Prof. Dr. Semir. A. Salim. Al Samarrai The Surgical treatment is one of the cornerstones of LUTS/BPO management. Based on its ubiquitous availability, as well as its efficacy, Monopolar-TURP has long been considered as the reference technique for the surgical management of LUTS/BPO. However, in recent years various techniques have been developed with the aim of providing a safe and effective alternative to Monopolar-TURP. The transurethral resection of the prostate (TURP) is performed using two techniques: monopolar TURP (M-TURP) and bipolar TURP (B-TURP). Monopolar transurethral resection of the prostate removes tissue from the transition zone of the gland. Bipolar TURP addresses a major limitation of M-TURP by allowing performance in normal saline. Prostatic tissue removal is identical to M-TURP. Contrary to M-TURP, in B-TURP systems, the energy does not travel through the body to reach a skin pad. Bipolar circuitry is completed locally; energy is confined between an active (resection loop) and a passive pole situated on the resectoscope tip (“true” bipolar systems) or the sheath (“quasi” bipolar systems). The various bipolar devices available differ in the way in which current flow is delivered [1,2]. Monopolar-TURP is an effective treatment for moderate-to-severe LUTS secondary to BPO. The choice should be based primarily on prostate volume (30-80 mL suitable for M-TURP). No studies on the optimal cut-off value exist, but the complication rates increase with prostate size [3]. The upper limit for M-TURP is suggested as 80 mL (based on the European Association of Urology Guidelines 2022 consensus, under the assumption that this limit depends on the surgeon’s experience, choice of resectoscope size and resection speed), as surgical duration increases, there is a significant increase in the rate of complications and the procedure is safest when performed in under 90 minutes [4]. Bipolar TURP in patients with moderate-to-severe LUTS secondary to BPO, has similar efficacy with M-TURP, but lower peri-operative morbidity. The duration of improvements with B-TURP were documented in a number of RCTs with mid-term follow-up. Long-term results (up to five years) for B-TURP showed that safety and efficacy are comparable to M-TURP [5-13]. The choice of B-TURP should be based on equipment availability, surgeon’s experience, and patient’s preference. The holmium laser enucleation of the prostate does not play a role in contemporary treatment algorithms, because there were no relevant publications on holmium laser resection of the prostate (HoLRP) have been published since 2004, HoLRP of the prostate. The thulium-aluminum-garnet laser (Tm:YAG) vaporization of the prostate has wavelength between 1,940 and 2,013 nm and is emitted in continuous wave mode. The laser is primarily used in front-fire applications [14]. Different applications such as vaporesection (ThuVARP) have been published [15]. As a limited number of RCTs with mid- to long-term follow-up support the efficacy of ThuVARP, there is a need for ongoing investigation of the technique. The transurethral incision of the prostate (TUIP) involves incising the bladder outlet without tissue removal. Transurethral incision of the prostate is conventionally performed with Collins knife using monopolar electrocautery; however, alternative energy sources such as holmium laser may be used [16]. This technique may replace M-TURP in selected cases, especially in prostate sizes < 30 mL without a middle lobe. The transurethral incision of the prostate is an effective treatment for moderate-to-severe LUTS secondary to BPO. The choice between M-TURP and TUIP should be based primarily on prostate volume (< 30 mL TUIP) [17]. The open prostatectomy is the oldest surgical treatment for moderate-to-severe LUTS secondary to BPO. Obstructive adenomas are enucleated using the index finger, approaching from within the bladder (Freyer procedure) or through the anterior prostatic capsule (Millin procedure). It is used for substantially enlarged glands (> 80-100 mL). The open prostatectomy is the most invasive surgical method, but it is an effective and durable procedure for the treatment of LUTS/BPO. In the absence of an endourological armamentarium including a holmium laser or a bipolar system and with appropriate patient consent, OP is a reasonable surgical treatment of choice for men with prostates > 80 mL. The bipolar transurethral enucleation of the prostate is a technology to enucleated the obstructive adenoma endoscopically by the transurethral approach. Bipolar-transurethral enucleation of the prostate (B-TUEP) evolved from plasma kinetic (PK) B-TURP and was introduced by Gyrus ACMI. The technique, also referred to as PK enucleation of the prostate (PKEP), utilises a bipolar high-frequency generator and a variety of detaching instruments, for this true bipolar system, including a point source in the form of a axipolar cystoscope electrode suitable for enucleation [18] or a resectoscope tip/resection loop [19, 20]. More recently, a novel form of B-TUEP has been described, bipolar plasma enucleation of the prostate (BPEP), stemming from B-TURP (TURis, Olympus Medical), that utilises a bipolar high frequency generator and a variety of detaching instruments including a mushroom- or button-like vapo-electrode [21,22] and a Plasmasect enucleation electrode [23] for this quasi-bipolar system. Bipolar transurethral enucleation of the prostate is followed by either morcellation [21,18] or resection [19-22, 24-26] of the enucleated adenoma. The holmium:yttrium-aluminium garnet (Ho:YAG) laser (wavelength 2,140 nm) is a pulsed solid-state laser that is absorbed by water and water-containing tissues. Tissue coagulation and necrosis are limited to 3-4 mm, which is enough to obtain adequate haemostasis [27]. Holmium laser enucleation of the prostate requires experience and relevant endoscopic skills. The experience of the surgeon is the most important factor affecting the overall occurrence of complications [28, 29]. Enucleation using the Tm:YAG laser includes ThuVEP (vapoenucleation i.e. excising technique) and ThuLEP (blunt enucleation). ThuLEP seems to offer similar efficacy and safety when compared to TURP, bipolar enucleation and HoLEP; whereas, ThuVEP is not supported by RCTs. Based on the limited number of RCTs there is a need for ongoing investigation of these techniques. The term minimal invasive simple prostatectomy (MISP) includes laparoscopic simple prostatectomy (LSP) and robot-assisted simple prostatectomy (RASP). The technique for LSP was first described in 2002 [30], while the first RASP was reported in 2008 [31]. Both LSP and RASP are
Benign Prostatic Enlargement قراءة المزيد »